NZ Herald: Health reform without the noise
As published in The New Zealand Herald, Saturday 27 June 2026
It is not often that meaningful change in New Zealand’s health system happens quietly.
Health is usually loud. It is political, personal and often understandably emotional. When things go wrong, they are felt quickly by patients, families, clinicians and communities. The pressure points are visible: long waits, stretched hospitals, difficulty getting a GP appointment, workforce shortages and the frustration people feel when the system does not work as it should.
But when things improve, progress can be harder to see. It can happen in policy settings, improved data collection and reporting, funding formulas, targets, operating models and infrastructure.
Right now, there are some positive changes happening in health that deserve to be acknowledged. They are not perfect. They will not fix decades of underinvestment overnight. But they are progressing. In a system as complex as health, progress matters.
One of the most important changes is the overhaul of the way primary care is funded.
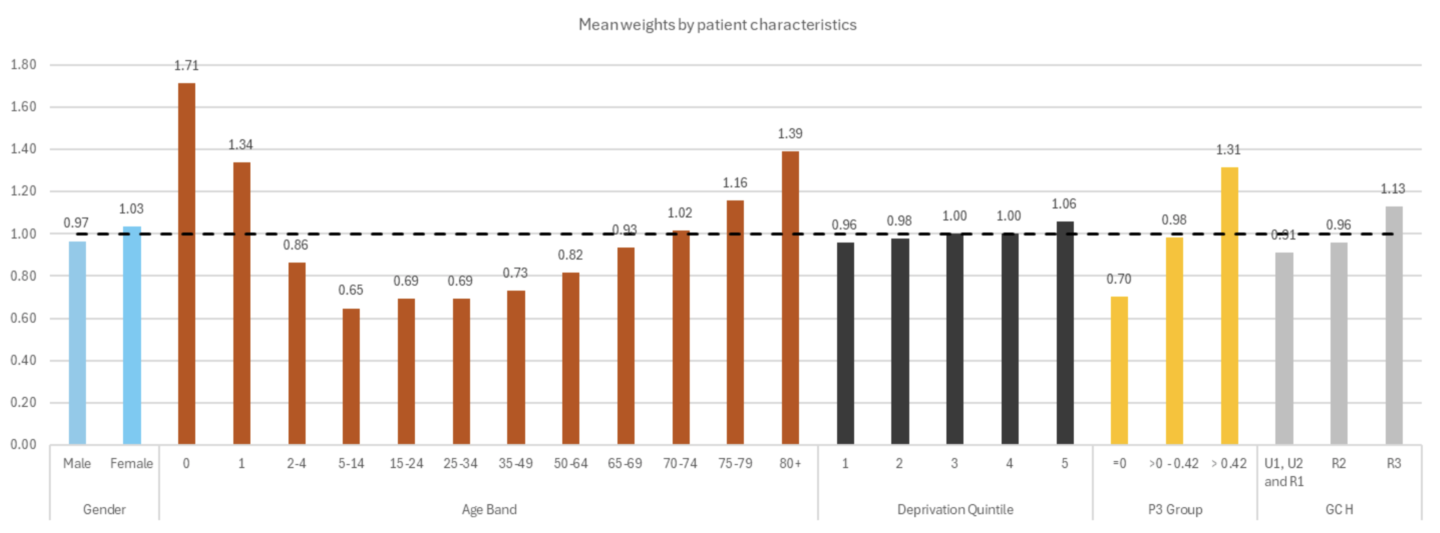
For nearly 20 years, New Zealand has used a capitation formula that has been widely accepted as too blunt. Capitation is the base funding general practices receive for enrolled patients, but the old model reduced a highly diverse population to just twelve possible funding amounts based on gender and six broad age bands. It did not properly reflect the reality that different patients, whānau and communities have very different levels of health need.
That matters because funding design drives behaviour. If funding does not reflect need, then the system risks underfunding the very communities that require more care, more outreach and more support. This is why the reweighting of capitation is important.
The new formula is not perfect. Ethnicity has not been included as a variable, which remains a significant issue given the persistent inequities experienced by Māori and Pacific peoples. There will also be winners and losers in any redistributive model.

But after two decades of talking about the need for change, the system has moved.
Credit should go to health officials and Health Minister Simeon Brown for progressing this important work. Overhauling a 20-year-old funding model is difficult and politically brave, particularly when any reweighting inevitably creates trade-offs. Audrey Young recently described Brown as “focused”, and this is a clear example of that focus being put to work on something that matters.
Nationally, Health New Zealand is investing an additional $128.4 million into primary care as part of this change. That matters. The reweighting is not just an academic exercise in funding design; it is backed by real investment into the part of the system where earlier care can make the biggest difference.
The new approach takes account of more detailed age bands, deprivation, rurality and multimorbidity, creating 1,080 different funding combinations. While that may sound complex, it means funding can be more precisely targeted to need. That is a meaningful shift towards funding care based on the complexity of patients’ lives, not simply the number of people enrolled.
It recognises that an 80-year-old with multiple long-term conditions may require far more care, follow-up and support than a generally healthy 65-year-old. It recognises that rural communities face different access challenges. And it recognises that deprivation has a direct impact on health outcomes, and should therefore be reflected in how care is funded.
That should be welcomed. It is also notable how little noise there has been around this change.
Often, health reform is accompanied by loud opposition, competing interests and sector tension. This change could easily have generated significant pushback because any reweighting of funding is, by definition, redistributive. Yet the relative lack of noise may reflect a quiet acceptance that the old system was no longer fit for purpose.
Primary care is the front door of the health system. It is where prevention happens. It is where early diagnosis happens. It is where chronic conditions are managed, medications are reviewed, children are immunised, mental health issues are first raised and many health problems are dealt with before they become hospital admissions.
When primary care works well, the whole system benefits. Patients get care earlier. Families have fewer crises. Hospitals are less pressured. Health outcomes improve over time. Properly funding primary care is not just good for general practice; it is one of the best investments we can make in the long-term sustainability of New Zealand’s health system.
The economics are clear. Keeping someone in a hospital bed overnight can cost around $7,000. Earlier intervention in primary care can often be delivered at a fraction of that cost, sometimes close to a tenth. That might mean treating an infection before it escalates, managing a chronic condition earlier or supporting someone before they end up in emergency care. It is better for patients, better for whānau and better for the taxpayer.
This is why primary care should not be seen as the cheap end of the health system. It is the smart end of the health system. It is where relatively small investments can prevent much bigger human and financial costs later.
This also matters in the context of the Government’s health targets.
Targets are not the whole answer. They can never capture the full humanity of healthcare or the complexity of patient need. But they do provide clarity. They tell the system what matters and where effort needs to be focused.
The current health targets focus on faster cancer treatment, improved childhood immunisation, shorter stays in emergency departments, shorter waits for first specialist assessments and shorter waits for elective treatment. These are areas that matter deeply to New Zealanders.
The latest results show year-on-year improvement across all five targets. The job is not done: too many New Zealanders are still waiting too long, and access remains uneven. But progress should not be dismissed simply because pressure remains. Both can be true.
There is also a new primary care access target due to take effect from July 2026. That is important. If we are serious about improving health outcomes, access to primary care needs to be measured, managed and improved with the same discipline as hospital performance.
A strong health system starts much earlier. It starts with reminders, recalls, screening, immunisation and proactive care. It starts with services that are easy for people to use, including people who have historically found the system hard to navigate.
That is why primary care reform matters so much. We should be honest about the scale of the challenge. But we should also be honest when progress is being made.
The shift in capitation funding, the focus on measurable health targets, increased investment in general practice, the development of online and after-hours options and work on shared health records all point to a health system slowly starting to modernise.
The real test will be execution.
Funding must reach the frontline. Targets must improve outcomes, not just reporting. Digital care must expand access without fragmenting continuity. Equity must be built into the system, not added later. And primary care must be treated as core infrastructure for New Zealand’s future health, not simply a pressure valve for hospitals.
In health, it is easy to focus only on what is broken. We must keep calling out gaps, delays and inequities, but we should not miss the moments where the system is beginning to shift.
Overhauling a 20-year-old funding system is progress. Clearer targets are progress. More investment in primary care is progress. Recognising patient need more accurately is progress. Modernising access to care is progress.
None of it is enough on its own, but it is a start.
The challenge now is to keep going: to build on the momentum, keep improving the model, ensure funding supports communities with the greatest need and keep primary care at the centre of the health system we need for the future.
New Zealanders deserve a health system that is easier to access, more equitable, more connected and more focused on keeping people well.
We are not there yet. But some of the foundations are beginning to move in the right direction, and that should give us reason for optimism.